
This image is taken from a study on identical twins, one of whom is a smoker.. the image is a split face- the( R ) side being from the non-smoker, the (L) side being from the smoker. for more info about how smoking damages *Effects Will Vary* see –Ways Smoking Affects Looks.
Smokers will develop more extensive and severe sun damage, due to the extensive degradation of metalloproteins or building blocks of collagen, plus the pro-carcinogenic effects of multiple chemicals present in cigarette smoke.
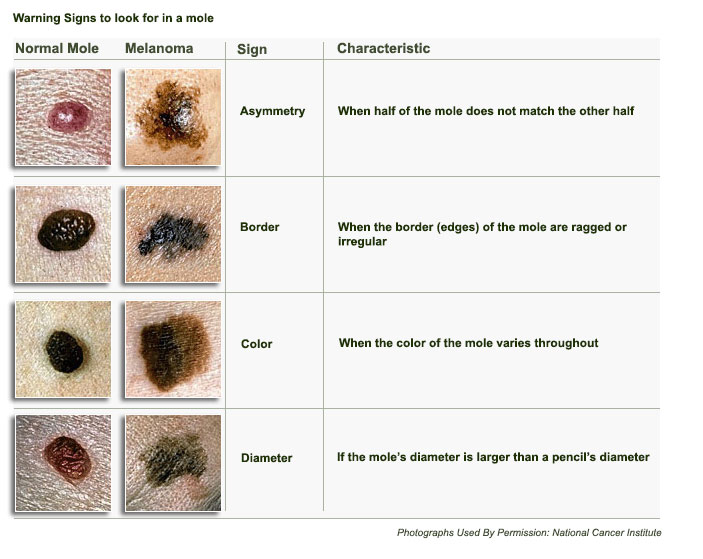
It is important to have a thorough inspection of areas where brown spots are present by a physician, as pigmented lesions can run the gamut from benign solar lentigines, seborrheic keratoses, through atypical melanocytic naevi to outright malignant melanoma.
Risk factors for skin cancer include multiple atypical naevi, a bad sunburn at a young age, use of sunbeds, family history of skin cancer.
1 in 7 Canadians will develop invasive skin cancer in their lifetime.
There are 3 main types of skin cancer
- Basal Cell Carcinoma– which is most frequently seen in the triangular area bounded by the nose and eyes, and typically looks like an ulcer with pearly edges;
- Squamous Cell Carcinoma- appears as rough or warty lesions, typically on the temples or backs of the hands.
- Malignant Melanoma, which looks like a mole, and can occur anywhere on the body. Danger signs to watch out for in a mole or freckle are:
- uneven or changing pigmentation
- enlarging size
- uneven borders or satellite lesions
- bleeding or itching
All suspicious lesions should be biopsied to rule out cancer.
At The Lazer Room, all patients are screened by Dr Hyland prior to treatments for brown spots, whether it be a series of AFA peels or IPL (intense pulsed light) or Fraxel Dual.
Examples of non-cancerous “brown spots” that are treated with other modalities:
Actinic Keratoses can spontaneously regress or can, in approximately 10% of cases, evolve into invasive squamous cell carcinoma: They are often found on exposed areas of skin, such as the back of the hands, or on the temples. Treatments include:
- Cryotherapy (freezing)
- Topical treatments: 5-fluorouracil cream, imiquoid
- Photodynamic therapy
- Thulium/Erbium Laser (see: Fraxel Dual)

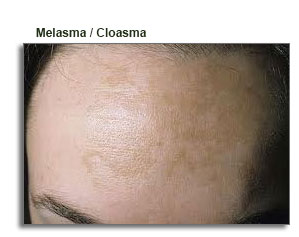 Melasma is a brown or bluish-grey skin discoloration typically seen in women age 25-50, occurring mainly on the upper cheeks, upper lip, forehead and chin, more common in women of Hispanic or Asian ethnicity, who have been exposed to strong sunlight, and is often associated with hormonal factors (pregnancy, birth control pills, or Hormone Replacement Therapy). The pigmentation is contained in the deep layers of the skin and responds poorly to IPL, great results are seen with Fraxel Dual Laser (see below). *Individual Results May Vary
Melasma is a brown or bluish-grey skin discoloration typically seen in women age 25-50, occurring mainly on the upper cheeks, upper lip, forehead and chin, more common in women of Hispanic or Asian ethnicity, who have been exposed to strong sunlight, and is often associated with hormonal factors (pregnancy, birth control pills, or Hormone Replacement Therapy). The pigmentation is contained in the deep layers of the skin and responds poorly to IPL, great results are seen with Fraxel Dual Laser (see below). *Individual Results May Vary
Melasma can be somewhat improved with glycolic or AFA peels. TCA peels have also been used, but the deeper peels carry the risk of post inflammatory hyperpigmentation.
Another approach is the use of over the counter or prescription bleaching creams, containing 2-4% hydroquinone*, azelaic acid, kojic acid, or retinoic acid.
These creams are often combined with topical steroids, to reduce skin irritation. Once the pigmentation is resolved, hormonal agents should be discontinued, and strict avoidance of sun exposure or the use of a high SPF sunscreen is recommended.
Some studies recommend pre-treatment for 8 weeks with a combination bleaching cream, followed by laser treatment. Thulium/Erbium (Fraxel Dual) is the most effective laser treatment to date, with an average of 3 treatments required.
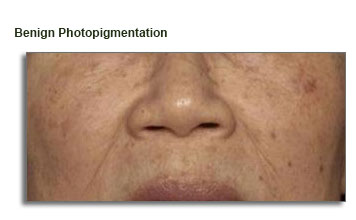
Occurs mostly on exposed areas of face, neck, chest and hands /forearms.
Treatment options
- Thulium laser (Fraxel 1927) is an incomparable new technology which specifically targets superficial pigmented lesions. One treatment will yield a remarkable improvement in pigmentation and skin texture, following a 2-3 day period of peeling.
Intense Pulsed Light (IPL) a series of 5-6 treatments 3-4 weeks apart will significantly reduce pigmentation by targeting melanin. the lesions will temporarily get darker; crusting or mild flaking will occur, followed by gradual improvement. Small blood vessels, or capillaries, in the treatment area may appear temporarily darker, or even bruise slightly, but will resolve over time. A secondary benefit – improved skin texture – through a temporary decrease in oiliness, pore size and an increase in collagen synthesis, has resulted in this treatment sometimes being referred to as a photofacial.
* Individual Results May Vary
